Dental Anxiety in Dental and Non-Dental Students
Abstract- Objective: To compare levels of dental anxiety in dental and non-dental students and then relate it with degree of knowledge about dental treatment procedures. Method: Modified Dental Anxiety Scale (MDAS) was used to measure and analyze statistically the dental anxiety among dental students (n=30) and non-dental students (n=30). The participants include 28 (46.7%) males and 32 (53.3%) females of age ranging from 18-24 years (mean age 21±1.619). The data was collected in Islamic International Dental Hospital, Islamabad from patients under waiting treatment. Results: Education was associated with dental anxiety in patients. The dental students had a mean dental anxiety score of dental students was found to be 13.5 and that of non-dental students was 16.5. Conclusion: The results support the hypothesis that knowledge about dental procedures has a significant role to elevate dental anxiety levels.
Keywords: dental anxiety; degree of knowledge; dental students; non-dental student
“Dental anxiety is an aversive psychological response to poorly define, or not immediately present dental stimulus interpreted as potentially harmful or dangerous, usually within a dental context”(
1
). Dental anxiety is a common phenomenon amongst patients prior to obtaining dental procedures, often giving rise to a vicious cycle of fear leading to avoidance of treatment(
2
,
3
). This potential hazard to treatment accounts for an understanding of its etiology, so as to help design and execute effective treatment regimens(
4
).Research establishes; prior experience of treatment, pain during treatment, age, gender, social class and lack of economic resources, negligence of oral health and inadequacy of and education as etiological factors of dental anxiety. Al-Omari et al. showed in their study that dental students had lowest anxiety levels as compared to medical and engineering students(
5
). Medical students were found to be the most anxious group and it was indicated that lack of dental information is directly related to increasing levels of dental fears. As per Curson and Coplans, anxiety is a major barrier in the dental treatments as children and adult avoid or delay attending the dentist except in emergency situations(
6
).Dental anxiety may have elevated levels amongst patients majorly due to lack of knowledge about the procedures and outcomes of dental treatment that would be carried out on them(
7
).Therefore, it is crucial to highlight dentally anxious patients in order to facilitate the course of treatment and to help accomplish it successfully. Different instruments for measuring dental anxiety include; Corah’s dental anxiety scale, Modified Dental Anxiety Scale (MDAS), Dental Fear Survey, State Trait Anxiety Scale, General Geer Fear Scale and Getz Dental Brief Survey(
1
). Humphris GM et al. (1995) suggested that MDAS is more comprehensive, highly valid and reliable, with a simpler and more consistent answering system(
8
).Therefore, modified dental anxiety scale has been used for the purpose of this study. The aim of the study was to understand how lack of knowledge of dental procedures may contribute to increased anxiety levels amongst non-dental students when compared to dental students. With the identification of existence of such differences, improved treatment techniques and management strategies may then be accomplished(
7
).
Materials and Methods:
The study was conducted at Islamic International Dental Hospital, Islamabad over a period of two months from May to June, on patients awaiting treatment while attending various departments at the hospital. This study is a cross- sectional study. Questionnaires were given to dental students (n=30) of first to fourth year (prior to receiving treatment) with their ages ranging from 18-24 years. Non-dental students (n=30) meeting the same age requirement were selected by purposive convenient sampling. The subjects were approached personally in clinical settings and questionnaire conducted after verbal consent. A total of 30 questionnaires were distributed to patients from each group. Data was obtained using modified dental anxiety scale, wherein extra items were added related to prior dental treatment experience and whether or not they had a dentist in their family. The modified dental anxiety scale consisted of five multiple choice items, including the following:
- If you had to go to your dentist for treatment tomorrow, how would you feel?
- If you were sitting in the waiting room (waiting for treatment), how would you feel?
- If you were about to have a tooth drilled, how would you feel?
- If you were about to have your teeth scaled and polish, how would you feel?
- If you were about to have a local anesthetic injection in your gum, how would you feel?
Options available as answers to each of the above question were ranging from not anxious scaled as 1 to extremely anxious scaled as 5. The scores of all the questions were summed up to give us the patient’s dental anxiety score. Demographic details in the questionnaire included age gender and education. For the statistical analysis data was studied using the statistical package for social sciences (SPSS) version 17.0. For descriptive analysis of data mean and standard deviation was computed for age. Calculation of dental anxiety scores was made to compare differences in level of anxiety amongst both the groups. If the total score of 15 or more was obtained, it was indicated that the subject was highly anxious(
9
).
Results:
|
|
|
|
DASCORE |
|
|
Mann-Whitney U |
238.500 |
|
Wilcoxon W |
673.500 |
|
Z |
-2.992 |
|
Asymp. Sig. (2-tailed) |
.003 |
|
a. Grouping Variable: Dental Student / Non-Dental Student |
|




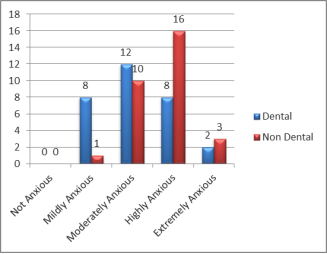
A total of 60 patients were included in this study; 30 dental students and 30 non-dental students. Out of this total of 60 patients, 28 (46.7%) were males and 32 (53.3%) were females. Their ages ranged from 18 to 24 years, giving a mean of 21 years with a standard deviation of ±1.619. There were 13 males (43.3%) out of a total of 30 dental students and 17 females (56.7%). In the non-dental category, there were 15 males (50%) and 15 females (50%) out of a total of 30 students. The results display that a total of 9 (15%) patients had mild anxiety, out of which 8(13.3%) were dental students and 1(1.7%) was a non-dental student. therefore it can be seen that anxiety levels among dental students correspond mainly to the lower level of mildly anxious. 22 (36.7%) of the total patients had a moderate category anxiety, out of these 12 (20%) were dental students and 10 (16.7%) were non dental students. 24 (40%) were highly anxious patients, out of those 2 (3.3%) were dental students and 3 (5%) were non dental students. There were no patients who showed a result of no anxiety levels (Fig.2). The graph for the mean dental anxiety scores of dental and non-dental students demonstrates a clear variation in the dental anxiety levels of the two groups. There is an increased average dental anxiety scores in non-dental students which urges the use of a statistical test to further analyze data. Accordingly the Mann- Whitney U test was undertaken. The p value obtained so forth was 0.003 which is less than the arbitrarily significant p value of 0.05, indicating a significant difference in DAS of the two groups. The (Fig.3) and (Fig.4) also,
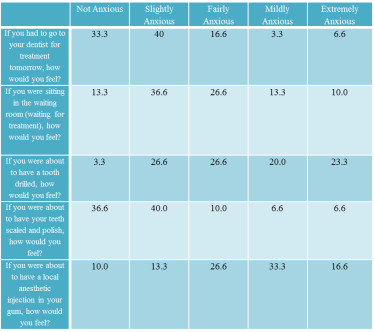
represent the percentage response in tabulated form.
Discussion:


The study was undertaken to examine the role of, awareness of dental procedures, on patient’s dental anxiety levels. The purpose of the study was to acquire an understanding of differences in the dental anxiety levels amongst patients with sufficient prior knowledge of dental procedures as in the case of dental students and those without. Realization of the existence of any such differences would help dentists design

strategies that would eliminate dental anxiety as a barrier to effective treatment. Dentally anxious patients often pose great difficulties during treatment(
2
).Such patients also are often resistant to going for treatment and may require behavioral pharmacological and educational interventions to allow for improved treatment and oral health statuses(
10
).The study was undertaken using the Modified Dental Anxiety Scale. The use of MDAS allowed for validity and reliability in the data collected thus serving as strength of the study(
8
,
11
). Standardization was also observed, with collection of all data in clinical settings. A major limitation of the study was its sample size. The survey comprised of only 60 patients, 30 being non-dental patients, receiving formal education in fields other than dentistry aged between 18-24 years. The second group comprised of dental students in any year of their study undergoing dental treatments and aged 18-24 years. The sample being selected randomly and by convenience also poses questions to generalizability of any findings as it is not representative of a much larger general

population. Dental anxiety is a vastly sought after topic with researchers attempting to understand its causative factors and its impact on oral health status of patients.

An in-depth understanding of its causative factors would enable practice of newer and improved techniques with increased patient compliance and willingness to undergo the required treatments without making the task difficult. Inadequate knowledge of dental procedure has also been studied as a causative factor of dental anxiety. Abu Hantash et al. suggested that dental anxiety in non-dental students is due to previous traumatic dental experiences and fear of pain(
12
,
13
).High levels of anxiety in non-dental students was also suggested due to lack of acquaintance with dental procedures(
14
,
15
).On the other hand enhanced education and awareness has been positively correlated to dental anxiety(
16
). B. Peretz et al. (1994) showed in his study that anxiety in dental students is inversely related to the exposure of dental procedures and it tends to reduce from preclinical to clinical years(
9
,
15
,
17
). Imran Farooq et al. (2014) following this study, found it sensible to deduce that dental anxiety in students declines with gradual progress in education and clinical exposure(
15
).Dental anxiety has been understood to have immense impact on oral as well as general health of individuals(
18
).Those who succumb to dental anxiety are found to enter a vicious cycle of ill-being. wherein anxiety leads to avoidance seeking treatment, leading to increased severity of disease and hence worsened oral and general health status(
19
), as shown in Fig.5. Some other important considerations that were beyond the scope of this particular study was an investigation of any previous traumatic dental experiences, especially from the non-dental students as they would have led to increased fears. Also there has been no ranking of anxiety provoking stimulus for dental students who may have been equally anxious about pain, and injection as is true of non-dental students. According to Todd and Walker(
20
), it was reported by 43% of people that they avoided going to the dentist lest they experienced increased troubles with their teeth. In another study by Curson and Coplans it was found that DA amongst both children and adult patients led to avoidance or irregularities in going for treatment, or visiting dentist in case of emergency only(6). The findings from our study prompt the need of devising ways to increase patient knowledge of procedures to decrease anxiety. This may include arranging of educational workshops on awareness about dental procedures.
Conclusion:
In conclusion there is existence of a difference in dental anxiety levels; among dental and non-dental students. With this difference it can be comprehended that dental anxiety owes itself to knowledge and awareness of dental procedures alongside other etiological factors. Know-how of dental procedures enhances patients’ ability to cope up with required treatment by eliminating barriers created due to anxiety. Hence increasing patient knowledge may serve to reduce apprehensions and enhance patient confidence on treatment procedure and its needs, consequently reducing anxiety.
References:
1.
http://www.st-andrews.ac.uk/dentalanxiety
.
2.Cooper CL WJ, Kelly M. Job satisfaction, mental health, and job stressors among general dental practitioners in the UK. British Dental Journal. 1987.
3.Armfield JM. What goes around comes around: revisiting the hypothesized vicious cycle of dental fear and avoidance. Community Dent Oral Epidemiol. Jun;41(3):279-87.
4.Taani DQ. Dental attendance and anxiety among public and private school children in Jordan. Int Dent J. 2002 Feb;52(1):25-9.
5.Al-Omari WM, Al-Omiri MK. Dental anxiety among university students and its correlation with their field of study. J Appl Oral Sci. 2009 May-Jun;17(3):199-203.
6.Curson I CM. The need for sedation in conservative dentistry. An investigation in the inner London area. 1970.
7.Appukuttan DP TA, Cholan PK, Subramanian S, Vinayagavel M. prevelance of dental anxiety among patient attending a dental educational institution in chennai, India. 2013.
8.Humphris GM, Morrison T, Lindsay SJ. The Modified Dental Anxiety Scale: validation and United Kingdom norms. Community Dent Health. 1995 Sep;12(3):143-50.
9.Peretz B, Zadik D. Dental anxiety of parents in an Israeli kibbutz population. Int J Paediatr Dent. 1994 Jun;4(2):87-92.
10.Marya CM, Grover S, Jnaneshwar A, Pruthi N. Dental anxiety among patients visiting a dental institute in Faridabad, India. West Indian Med J. Mar;61(2):187-90.
11.Corah NL. Development of a dental anxiety scale. J Dent Res. 1969 Jul-Aug;48(4):596.
12.Abu Hantash AY, Al Aker Dental Anxiety and Fear among medical field students at Al Quds University
13.Mohammed RB, Lalithamma T, Varma DM, Sudhakar KN, Srinivas B, Krishnamraju PV, et al. Prevalence of dental anxiety and its relation to age and gender in coastal Andhra (Visakhapatnam) population, India. J Nat Sci Biol Med. Jul;5(2):409-14.
14.Serra-Negra J, Paiva SM, Oliveira M, Ferreira E, Freire-Maia F, Pordeus I. Self-reported dental fear among dental students and their patients. Int J Environ Res Public Health. Jan;9(1):44-54.
15.Imran Farooq SA. A cross sectional study of gender differences in dental anxiety prevailing in the students of a Pakistani dental college. 2014.
16.Kirova DG, Atanasov DT, Lalabonova CK, Janevska S. Dental anxiety in adults in Bulgaria. Folia Med (Plovdiv). Apr-Jun;52(2):49-56.
17.Peretz B, Mann J. Dental anxiety among Israeli dental students: a 4-year longitudinal study. Eur J Dent Educ. 2000 Aug;4(3):133-7.
18.McGrath C, Bedi R. The association between dental anxiety and oral health-related quality of life in Britain. Community Dent Oral Epidemiol. 2004 Feb;32(1):67-72.
19.Attaullah AAK. PREVALENCE OF DENTAL ANXIETY AMONG UNIVERSITY
STUDENTS IN ISLAMABAD, PAKISTAN.
20.Todd JE WA. Adult Dental Health in England and Wales. 1980
PLACE THIS ORDER OR A SIMILAR ORDER WITH NURSING TERM PAPERS TODAY AND GET AN AMAZING DISCOUNT
