Epidemiological Patterns of Gestational Diabetes by Person, Place, and Time
Gestational diabetes is a common health condition that affects pregnant women worldwide. Gestational diabetes is defined by the American Diabetes Association as a woman without diabetes developing high blood glucose sometime during pregnancy. According to an article by Lavery, Friedman, Keyes, Weight, and Ananth (2016), “gestational diabetes is a condition which affects around 8.3% of pregnancies worldwide.” Gestational diabetes is a growing public health problem as women becoming pregnant are increasingly overweight or obese and as maternal age at conception increases.
As mentioned previously, gestational diabetes is a growing problem worldwide. Gestational diabetes is a health condition which affects women of childbearing age (person). However, the effects of gestational diabetes may be seen in women who are no longer of childbearing age who had gestational diabetes during a pregnancy earlier in life. Gestational diabetes may also affect the infant born to a mother with this condition as gestational diabetes can lead to adverse outcomes in prenatal development. When blood glucose is not controlled in pregnancy the outcomes may include a baby that is large for gestational age (LGA), high blood pressure or resulting pre-eclampsia, hypoglycemia in the infant following birth, and a potential cesarean section for delivery which may result in a longer recovery time following delivery (Centers for Disease Control and Prevention, 2018). According to Lavery, Friedman, Keyes, Weight, and Ananth (2016), stillbirth has also been a risk factor in relation to gestational diabetes. Women with gestational diabetes during pregnancy are also at greater risk for developing type II diabetes mellitus in the future. Gestational diabetes is also a public health problem in that this is costly to the health care system to treat women and children with complications from gestational diabetes.
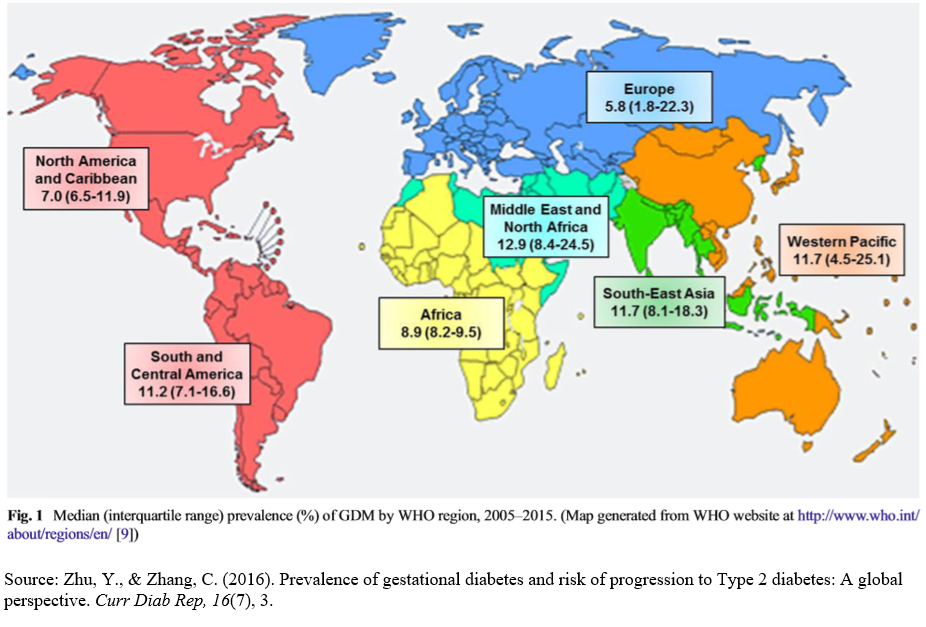
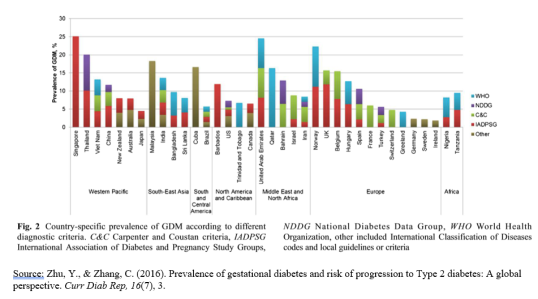
Gestational diabetes is becoming an increasing global burden as countries are becoming more developed (place). According to Zhu and Zhang (2016), the prevalence of gestational diabetes has been increasing by over 30% in the last two decades in developing countries worldwide. In this study, data was collected from 36 countries to account for gestational diabetes rates. This study found that the Middle East, as well as North Africa, had the highest rates of gestational diabetes with the median rate being 12.9% for these locations. The lowest prevalence of gestational diabetes was found to be in Europe with a median incidence of gestational diabetes being 5.8% (Zhu & Zhang, 2016). Gestational diabetes will continue to be a growing problem
worldwide as countries become increasingly sedentary, maternal age increases, and obesity continues to be a global health problem.
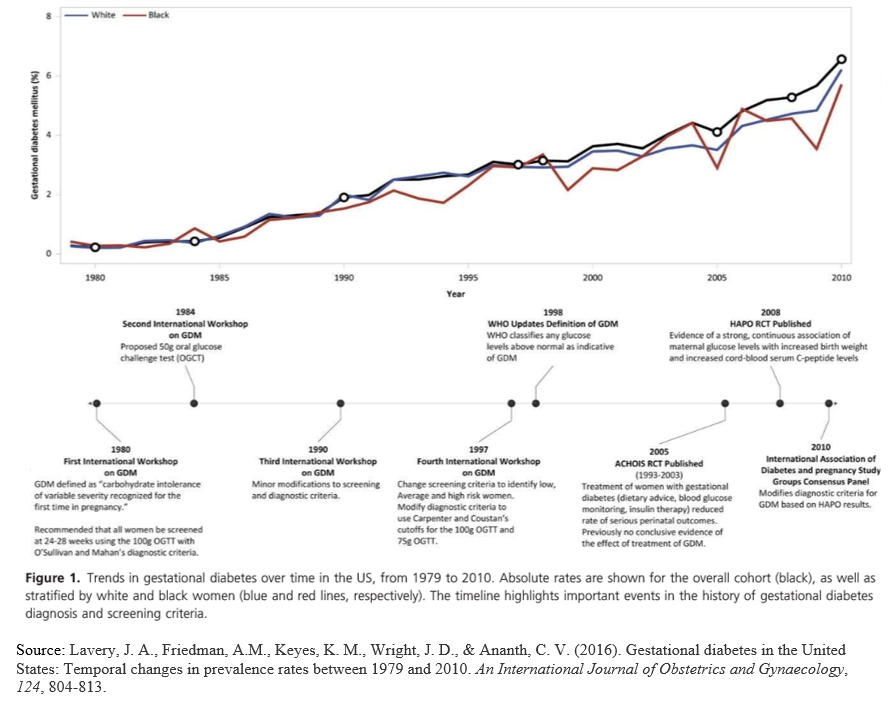
Gestational diabetes is not usually diagnosed until later in pregnancy as it is generally tested for between 24 to 28 weeks of gestation (time) (Centers for Disease Control and Prevention, 2018). Gestational diabetes is different than type I diabetes mellitus or type II diabetes mellitus in that it is classified as pregnant women who did not have diabetes prior to conception. Trends in gestational diabetes have increased in the United States over time from 1980 to 2010 as depicted in the figure below (Lavery, Friedman, Keyes, Weight, & Ananth, 2016). All pregnant women should be screened at some time their pregnancy for gestational
diabetes, as there are multiple complications of untreated gestational diabetes. According to the National Institute of Diabetes and Digestive and Kidney Diseases (2017), there are different ways that a practitioner may diagnose gestational diabetes; the glucose challenge test, oral glucose tolerance test (OGTT), or both tests. The glucose challenge test consists of a blood draw one hour following the pregnant woman drinking a glucose solution. If the measurements from this test determine that blood glucose is 140 or higher the woman may need to come back for an OGTT. If the blood glucose is measured at 200 or higher the woman may be diagnosed with gestational diabetes (National Institute of Diabetes and Digestive and Kidney Diseases, 2017). If the woman needs an OGTT, she will first have a blood draw performed, drink the glucose solution, then undergo subsequent blood draws every hour for two to three hours. High blood glucose levels at any of the blood draws for this test would be indicative of gestational diabetes (National Institute of Diabetes and Digestive and Kidney Diseases, 2017).
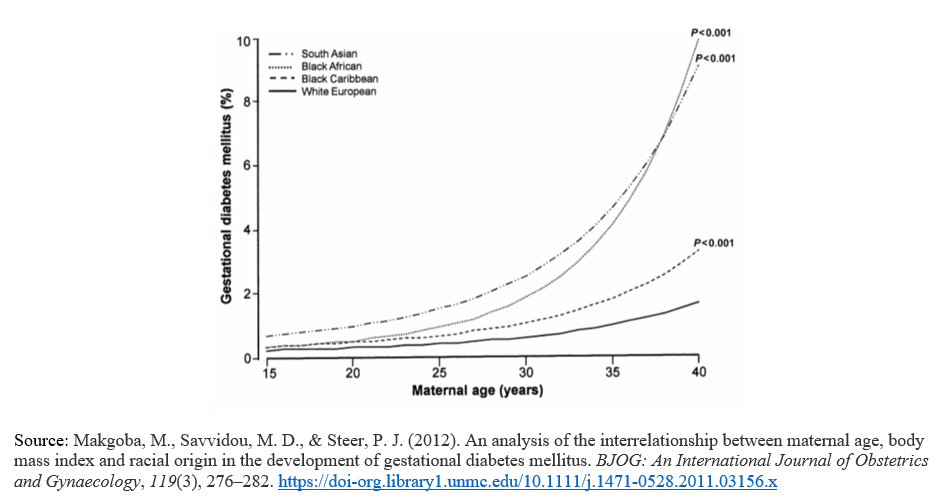
As with most conditions, there are risk factors that predispose women to have gestational diabetes in pregnancy. According to a study by Poomalar (2015), some high risk groups of women at risk for developing gestational diabetes include high body mass index (BMI), having a first degree relative with diabetes mellitus, having a previous infant born with macrosomia, having a history of gestational diabetes in previous pregnancies, and women of certain ethnic descent including individuals from Asia, the Caribbean, Arabia, and the Middle East. There has also been a linkage to maternal age and the development of gestational diabetes during pregnancy. According to Makgoba, Savvidou, & Steer (2012), increasing maternal age and BMI are greater risk factors for the development of gestational diabetes in South Asian and Black African women compared to White European or Black Caribbean women (see graph). There has also been some discussion that maternal diet plays a factor in the development of gestational diabetes during pregnancy as there are food choices that are obvious in leading to increased blood glucose.
There have been many prevention and control measures that have been studied in regards to gestational diabetes. The Centers for Disease Control and Prevention (2018) offers many prevention and control tips for women at risk for or who have gestational diabetes. These tips include eating healthy foods which may include getting help from a registered dietician, exercising regularly to include at least 30 minutes of moderate-intensity exercise at least five days per week, monitoring blood glucose levels as directed by a practitioner, taking insulin if prescribed, and getting tested for diabetes mellitus following pregnancy. There is also current studies to determine if probiotics and vitamin D help aid in the prevention of gestational diabetes (Poomalar, 2015). Women who with a past history of gestational diabetes should work on future prevention prior to subsequent pregnancies through the methods mentioned above.
In conclusion, gestational diabetes is becoming an increasing global health risk. It is a health condition that may affect any women of childbearing age who is pregnant, plans to become pregnant, or has been pregnant. It may also impact a developing fetus as well as an infant born to a mother who had gestational diabetes during that pregnancy. Gestational diabetes occurs worldwide, though there is a higher prevalence in some ethnicities than others (as mentioned previously). There are many risk factors that may predispose women to develop gestational diabetes and fortunately, there are also many prevention and control measures to reduce these risk factors. More work will be needed in public health outreach to helping women become more aware of these risks as well as the implementation of primary prevention measures to decrease the incidence of this condition worldwide.
Evaluation of Data Sources
Centers for Disease Control and Prevention:
The Centers for Disease Control and Prevention has ample information available regarding public health diseases including gestational diabetes. There is data available about rates, prevention measures, risk factors, and numerous other information sets regarding gestational diabetes on this site. The CDC uses the National Notifiable Diseases Surveillance System (NNDSS) to gain information from local and state health departments. The strengths of using this source are that this is information obtained from the CDC is reliable and lacks the bias that some research studies or other internet sources may have. I used this data source because it was helpful in that the CDC sets primary prevention measures which fit well into my rationale for prevention and control measures for gestational diabetes. I also enjoy the CDC data because it is at a level that individuals that do not have public health or medical background can understand. This is imperative due to the fact that the CDC sets many guidelines for disease and illness prevention.
Lavery, Friedman, Keyes, Wright, & Ananth:
This is a research article that I obtained through EBSCO (UNMC library) which talks about the prevalence and risks of gestational diabetes. This is a retrospective cohort study from 2016. The strengths of this research article were that it was clear and concise, had no outside funding which helped to ensure that bias is limited, and this study used a cohort of women with many different variables (varied ages, races, marital status, etc.). This study was also from a peer-reviewed journal (
BJOG: An International Journal of Obstetrics and Gynaecology).
However, this study did not disclose interests or limitations. I chose to use this research article for my project because it had great evidence-based recommendations and used epidemiologic patterns and definitions that I could understand. This article also had a lot of interesting information regarding maternal trends related to gestational diabetes which were actually hard for me to find from many of the other sources. Lastly, I used the figure from this study because it did a great job at comparing different races of women with gestational diabetes, but also had a timeline of why the rates of gestational diabetes rates are increasing over time.
Makgoba, Savvidou, & Steer:
This is a research article that I obtained through EBSCO (UNMC library) and is a retrospective study from 2012. This study looked at multiple factors in relation to gestational diabetes which includes maternal age, body mass index (BMI), and race of the mother. This study was from the same peer-reviewed journal as the previous study I mentioned (
BJOG: An International Journal of Obstetrics and Gynaecology
). The strengths of this research article were that the data collection methods were very clear, statistical analysis was done in a way that I could clearly comprehend, there was no outside funding source limiting bias, and I liked that the results were depicted in a linear fashion. I also liked that this study looked at BMI in with maternal age and race in that high BMI’s correlating to overweight and obesity do have a large role in gestational diabetes development. A limitation of this data source was that it was retrospective so data was collected from women who were self-reporting these factors and this may lead to inconsistency with screening. I chose to use this data because I liked the data and how there was a combined link between the factors of maternal age, BMI, and maternal race. This helped me in realizing that there are multiple factors often acting in conjunction in the development of diseases including gestational diabetes.
National Institute of Diabetes and Digestive and Kidney Diseases:
The National Institute of Diabetes and Digestive and Kidney Diseases is a program funded by the National Institute of Health (NIH) which conducts medical research regarding endocrine and metabolic disorders inclusive of gestational diabetes. This data is available to the public and has an aim to increase knowledge and understanding of endocrine and metabolic disorders. The strengths of this data are that this information is reviewed by experts (much like the data from the CDC), the aim is to help the general public so the information is easy to read and understand, and there is a wealth of great information regarding gestational diabetes. A limitation of this source is that often the data has to be written at a level the general public can understand (general rule is fifth-grade level), so there is not a lot of statistical data for this source. I chose to use this source because of the data regarding testing for gestational diabetes. I am currently pregnant and the information that is given on this site is the same information that I was given in a handout by my midwife.
Poomalar:
This is a journal article written in a 2015 edition of the
World Journal of Diabetes
. This article depicts management and trends in gestational diabetes. This article starts by speaking about the trends in gestational diabetes and later talks about prevention and treatment for gestational diabetes. The strengths of this article are that it is organized well into sections explaining the prevention, diagnosis, and treatment of gestational diabetes, there were no reported conflicts of interest and was peer-reviewed by external reviewers. A limitation of this article is that it did not include a lot of statistical data or graphical data to explain epidemiological trends. I chose to use this article because I really liked how it broke up the different information about gestational diabetes, and I like that it very clearly represented the different prevention and treatment methods for gestational diabetes. It also depicted some prevention measures that are currently being studied like probiotics and vitamin D supplementation. I also felt as though this was a reputable source coming from the
World Journal of Diabetes
as well as the fact that this article was peer-reviewed.
Zhu & Zhang:
This was a systematic review which looked at the global prevalence of gestational diabetes as well as the progression from gestational diabetes to type II diabetes mellitus. I information from this article was obtained from collecting different data sources through research articles from different countries. The strengths of this article are that it shows rates of gestational diabetes worldwide, depicts that there is a direct linkage between women who have gestational diabetes and the linkage of developing type II diabetes mellitus in the future, and depicts public health implications of both gestational diabetes and type II diabetes mellitus. I also liked the way that the world map showed the prevalence of gestational diabetes between different regions of the world. A limitation of this study was that it was hard to follow at times and would be difficult to distinguish the data if the reader did not have knowledge regarding healthcare statistics or epidemiology. I chose to use this study in my project because of the information it depicted comparing the prevalence of gestational diabetes among different countries and regions, as the majority of my other sources only had information regarding the prevalence of gestational diabetes in the United States.
References
-
Centers for Disease Control and Prevention. (2018).
Gestational diabetes and pregnancy.
Retrieved from
https://www.cdc.gov/pregnancy/diabetes-gestational.html
-
Lavery, J. A., Friedman, A.M., Keyes, K. M., Wright, J. D., & Ananth, C. V. (2016). Gestational diabetes in the United States: Temporal changes in prevalence rates between 1979 and 2010.
An International Journal of Obstetrics and Gynaecology, 124,
804-813. -
Makgoba, M., Savvidou, M. D., & Steer, P. J. (2012). An analysis of the interrelationship between maternal age, body mass index and racial origin in the development of gestational diabetes mellitus.
BJOG: An International Journal of Obstetrics and Gynaecology
,
119
(3), 276–282.
https://doi-org.library1.unmc.edu/10.1111/j.1471-0528.2011.03156.x
-
National Institute of Diabetes and Digestive and Kidney Diseases. (2017).
Tests & diagnosis for gestational diabetes.
Retrieved from
https://www.niddk.nih.gov/health-information/diabetes/overview/what-is-diabetes/gestational/tests-diagnosis
-
Poomalar, G. K. (2015). Changing trends in management of gestational diabetes mellitus.
World
Journal of Diabetes
,
6
(2), 284–295.
https://doi-org.library1.unmc.edu/10.4239/wjd.v6.i2.284
-
Zhu, Y., & Zhang, C. (2016). Prevalence of gestational diabetes and risk of progression to Type 2 diabetes: A global perspective.
Curr Diab Rep, 16
(7), 1-11.
PLACE THIS ORDER OR A SIMILAR ORDER WITH NURSING TERM PAPERS TODAY AND GET AN AMAZING DISCOUNT
